Schools have just reopened. The new term promises something different for students from Grades 6-13 who reportedly will be expected to follow a ‘Sareera Suwatha’ ( School Physical Well Being ) programme every morning before they start their class work. Health officials have collectively hailed this as a good move on the part of the present Good Governance Government due to the sharp rise in avoidable non communicable diseases caused prematurely by the lack of physical exercise in schoolchildren. Preference for non active sedentary activities such as, watching T.V, playing computer games and even doing classroom assignments on line has put outdoor sports and games to a position of low priority as never before. By placing physical activities in the highest run of priority with the ‘Sareera Suwatha’ programme, health officials are confident it would help increase the physical development of the growing child, reduce obesity, stimulate blood cells and in general help millions of schoolchildren to stay fit and healthy.
However, they also warn that pushing children to exceed their limits and acceptable thresholds while exercising or playing active games can also have its drawbacks. This is especially so in knee problems that most adolescent children experience at this stage of their lives when their bones are still growing rapidly. One of the commonest, we learned is an ailment, medically called Osgood Schlatter’s disease. A self-limiting syndrome, which occurs more frequently in boys from 11-15 years, than in girls, due to their greater participation in sports with male-to-female ratio reportedly ranging from 3:1 to as high as 7:1., the good news is that it is treatable and will completely go away by the child’s 16th birthday. No radical treatment is required. Gentle exercises under the supervision of a qualified physiotherapist and heat treatment can relieve the pain and help the victim to cope with this temporary phase.
The Sunday Observer spoke to Chartered Physiotherapist Dr Gopi Kitnasamy who draws from his three decades of experience in treating students with this condition and other knee problems to share some valuable insights with our readers. He also tells us how obesity and poor diets are linked to knee problems in children, and advises parents to encourage children to exercise more and eat healthier meals.
Excerpts..
 Q. Schools have now reopened for the second term and most children are back to their usual classroom activities. In addition, children from Grades 6-13 in all curriculum streams are now expected to follow a ‘Sareera Suwatha’ (School Physical Well being) program every morning, before they begin their class work. Is this a good thing?
Q. Schools have now reopened for the second term and most children are back to their usual classroom activities. In addition, children from Grades 6-13 in all curriculum streams are now expected to follow a ‘Sareera Suwatha’ (School Physical Well being) program every morning, before they begin their class work. Is this a good thing?
A. Yes it is. Outdoor activities form an important part of their life and have long term benefits on their health. Adequate outdoor activity increases health and physical development by improving sensory development, reducing obesity and stimulating blood cells. It helps kids stay fit and active which will benefit them in the long run. They can ward off health problems like obesity and heart ailments later in life. Participation in sports activities improves physical fitness, coordination, and self-discipline, and gives children a valuable opportunity to learn teamwork.
Q. In many instances, these programmes lack qualified physiotherapists and instructors who could guide students on developing fundamental movement skills. Could this cause harm to some specific parts of their bodies? Which part/s of the body are most exposed to injury due to this oversight?
A. Kids can be particularly at risk of sports injuries for a variety of reasons because they are still growing and developing. Treating sports injuries is often difficult, expensive and time consuming, and thus, supervised and guided sports can prevent sports injuries. The parts of the body commonly affected are the shoulder, knee and ankle.
Q. If you look at the gender and age of the children most at risk, who are more vulnerable, males or females, and at what age?
A. Boys are prone to more injuries than girls and more severe ones like head injuries, fractures and dislocations. The type of injuries may vary depending on the age and the sport. Ankle and knee injuries are common among the girls; while shoulder, elbow, spine and head injuries are more common among the boys.
Q. I understand, there is a specific knee pain said to be common in adolescent children, mostly young boys, called Osgood-Schlatter disease knee pain. Is this commonly found in young boys in Sri Lanka as well? What is the approximate incidence judging by the number of adolescents who come to your clinic for treatment?
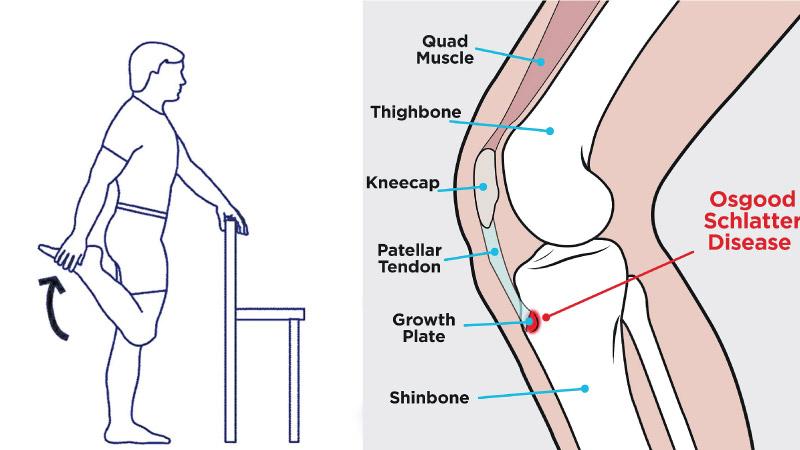
A. Osgood-Schlatter disease is an inflammatory injury of the growth plate on the tibia (shin bone) just below the level of the knee at the tibial tubercle . The tibial tubercle is the bony attachment for the quadriceps (front thigh muscle). This is a very important muscle which helps in getting up from seated position, walking, climbing, running, jumping, etc. It is an overuse knee injury rather than a traumatic injury. This condition usually strikes adolescents who are active during their growth spurts, which is the two year period where they grow most rapidly. It is more common in boys but can affect either gender if the children are active. Tight thigh muscles are also predisposed to this disease. The most prevalent groups are Boys: ages 11-15 – Girls: ages 8-13.
Q. How is it caused?
A. A growth plate is an area of developing tissue near the ends of long bones or areas of muscle attachment. The growth plates in children allow the bones to expand in length thus allowing a child to reach his or her full height by the age of 16 to 19. During a growth spurt in a child, the lengthening of the muscle is unable to keep up with the lengthening of the rapidly lengthening femur, resulting in an increased pulling force on the tibial tuberosity. Activities involving repetitive, strong quadriceps contractions, such as, in jumping, running, volleyball, basketball, soccer, gymnastics, dance, rugby and netball are most at risk.
 Q. Why is it that more males are affected by it than female adolescents?
Q. Why is it that more males are affected by it than female adolescents?
A.. It has been suggested that the difference is related to a greater participation by boys in sports and risk activities, than by girls.
Q. Is it a permanent condition? Will it eventually go away when the adolescent attains manhood?
A. Osgood Schlatter’s disease is a self-limiting syndrome. Complete recovery can be expected with the closure of the tibial growth plate. Complications of this condition include a persistence of a bump overlying the tibial tubercle, reoccurrence in adulthood, tearing away (avulsion) of the growth plate from the tibia.
Q. How is it detected? Is it visible on the outside e.g. is there redness or swelling?
A. Pain is the leading symptom in this disease and it appears and aggravates during physical activities such as, running, jumping, cycling, kneeling, walking up and down the stairs and kicking a ball (knee straightening). Pain is localised to the area of the tibial tubercle, the tubercle may be swollen, and tightness of the quadriceps muscle are the common symptoms. It can normally be diagnosed without the need for further investigation. Plain X-rays are commonly taken to rule out other conditions such as, a tibial tuberosity fracture, malignancy, or infection.
Q. How is it treated? What is the first line of treatment and thereafter what needs to be done?
A. Initial treatment of this injury consists of modification of activities, applying ice, stretching, strengthening exercises, and pain medications. Immediate restriction of high impact activities such as, jumping and running. Use an infrapatellar knee strap to dissipate forces away from the tibial tubercle. Kinesiology or K taping may provide both pain relief and load reduction at the site of pain and injury. Ice should be applied for 10-15 minutes to the affected knee every 2 to 3 hours as needed to help reduce inflammation and pain.
Q. Is surgery necessary at any point?
A. Surgery is rarely required and if needed, is done only in adults, as the disease usually resolves itself in children and surgery could damage the growth plate area. The surgery removes the bone fragments that are causing irritation of the tendon. By removing the bone fragments, the knee is able to function fully without the pain the disease causes.
Childhood obsesity and overweight are two big problems that are of concern to health authorities since they lead to several diseases early in life such as type 2 diabetes mellitus , hypertension and dyslipidemia.
Q. Is childhood obesity linked to knee pain and other joint related pains in children?
A. Yes, childhood obesity is one of the main risk factors in getting this condition, as extra body weight puts more stress on the knee.
Q. Lack of exercise is also said to be a key contributor to the poor state of physical health of most children and adolescents. This is because most children have turned outdoor recreation into indoor recreation with screen watching and computer games. Your comments?
A. Lack of physical exercise in children is the main culprit in the startling rise of childhood obesity, heart disease, diabetes, and all other types of preventable medical conditions. Other behaviours that influence excess weight gain include eating high-calorie, low-nutrient foods and beverages, sedentary activities such as, watching television or other screen devices and sleep routines.
Q. What kind of exercise do you recommend?
A. The physiotherapist will focus on exercises to improve the flexibility and strengthen the surrounding musculature. This includes the quadriceps, hamstring, iliotibial bands and the gastrocnemius muscle. High-intensity quadriceps-strengthening exercises increase stress across the tibial tubercle and are initially avoided. Stretching should initially be performed to reduce the tightness in the quadriceps muscle. Low-intensity quadriceps-strengthening exercises, such as isometric exercises, are very important to condition the muscle. High-intensity quadriceps strengthening exercises and hamstring stretching are introduced gradually.
Q. There have been times when students participating in inter house sports are forced to continue playing even when they complain of knee pain. What could be the result of this?
A. The growing concern is that many of these children ignore their injuries, and such inattention can worsen the issue over time. Another trend is that kids focus more on just one sport to become ultra-competitive. As a result, many of them are pushing themselves beyond acceptable thresholds which may lead to repetitive injury and eventually more serious functional loss and force you to get out of your sport.
Q. Any dietary guidelines? Some children come on empty stomachs and exercising on an empty stomach could nullify the positive effects of morning exercise. The Education Ministry has now started a programme of giving children a cup of nourishing milk and breakfast which is showing good results. Your comments.
A. Breakfast is the most important meal of the day. “Breaking the fast” has long been promoted as a healthy way to start the day. Eating a healthy breakfast before starting the school day is linked to improved concentration, better test scores, increased energy, a higher intake of vitamins and minerals, and even a healthier body weight. Skipping breakfastcan make kids feel tired, restless, or irritable. Their mood and energy may drop by mid morning, and it could affect a child’sperformance on the sporting field as well as affect their growth and development. Also, it’s important for young athletes to drink plenty of fluid to prevent dehydration.
Q. What is your advice to parents on this subject?
A. Today, there is no need for total immobilisation, or for totally refraining from athletic activities. The most important thing is that the parents, the coach, and the child should be aware of the natural course of this disease. The child should continue his normal physical activities, to the limit that the pain allows it, so lower the intensity of frequency of exercising (activity modification). Swimming is a secondary athletic activity, and is a good alternate until this condition settles.