







Dr. Chin Chong Min, senior consultant urologist and Robotic surgeon attached to the Mount Elizabeth Novena Hospital, Singapore in an interview with the Sunday Observer discussed the risk factors for Prostate cancer and the importance of preventive measures such as undergoing a PSA test starting at age 50. Dr. Chin elaborated on the latest treatment options available, including robotic surgery.
Dr. Chin was in Sri Lanka recently to attend a medical seminar organised by Sri Lankan urologists.
Excerpts
Q: The two key risk factors for prostate cancer are diet (including animal fat) and age. On what are the risk factors based?
 A: The risk factors are based on epidemiological / population studies which showed higher cancer rates correlate with consumption of animal fat. Westerners have a higher animal fat consumption (such as milk, and beef.) Hence the rate in these Western countries is higher than in Asia. But we are fast catching up given our diet changes to meat.
A: The risk factors are based on epidemiological / population studies which showed higher cancer rates correlate with consumption of animal fat. Westerners have a higher animal fat consumption (such as milk, and beef.) Hence the rate in these Western countries is higher than in Asia. But we are fast catching up given our diet changes to meat.
In the USA, the African blacks who migrated there have an even higher cancer rate than the Caucasian Whites. The higher rates with age come from the Cancer Registry which shows a huge jump in cancer in men above 65 years. This reinforces age as a risk factor. Finally, there is the genetic factor which accounts for only 9 percent of cases and explains cancer seen in men < 60 years and cancers within the family lineage. Genetic cancers tend to be of a more aggressive type too.
Q: Considering that age and dietary habits are major risk factors for prostate cancer, what precautionary measures can men take to reduce their risk of developing this disease?
A: A diet change to less fat and more vegetables is highly recommended as we can’t stop the process of ageing nor change our genes. Hence, this is not enough to “protect” men from getting prostate cancer. The next best way is early detection. Fortunately, we have a tumour marker called the PSA and such screening can begin at the age of 50 years.
Q: The cure rate for prostate cancer is 95 percent, but early diagnosis is required. Could you tell us more about the stages of prostate cancer and the cure rate at each stage?
A: As with all cancers, the highest cure rates are achieved if the cancer is in stage 1.
The stages are as follows;

Dr. Chin Chong Min
In Stage 1, there are no symptoms. The cancer is small in volume and cannot be felt with the finger. It is diagnosed at health screening when a high PSA level (> 4 ng/dl) is found.
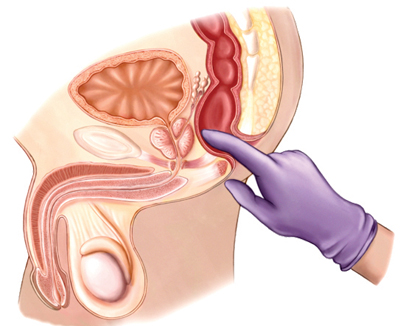
In Stage 2, prostate cancer can be felt as a hard nodule on rectal examination. Although the cancer is bigger, it is still confined within the prostate, and cure is still possible.
By Stage 3, the cancer has spread out of the prostate capsule. Common symptoms at this stage include difficult urination. This is now at a locally advanced stage and carries a lower chance of cure. Treatment is aimed at slowing its spread and preventing bladder blockage.
The PSA level is usually > 10 ng/dl at this stage.
At Stage 4, the cancer has already spread beyond the prostate to the lymph nodes and bones. Symptoms at this stage include difficult urination, bone pain, weight loss, and fatigue. At this stage, treatment is targeted at preventing further complications and reducing pain. The PSA level is usually > 100 ng/dl by now.
Q: What are the common symptoms, and at what stage do they appear?
A: In the early stages, there are no symptoms as the cancer is too small. The PSA level tends to be < 10 ug/L in these cases. Once the cancer reaches
Stage 3, the symptoms are similar to BPH. The PSA then tends to be > 20 ug/L. PSA is a good correlation to stage – the higher the PSA, the more advanced the stage.
Q: How many types of PSA Tests are there?
 A: There are 3 types of PSA Tests. The Total PSA can be done for initial screening purposes. Most guidelines propose at the age of 50 years, although some recommend 45 years if there is a strong family history of cancer. If it is above 4 ug/L, then the test can be repeated to include the Free/Total PSA. However, if available, I prefer to do the PHI test (Prostate Health Index) which includes the Total PSA, Free PSA, and the PHI score. A score above 50 is highly suspect of cancer. The problem with PSA is that it can also be raised in those with large benign prostates (BPH) as well as prostatitis (inflammation).
A: There are 3 types of PSA Tests. The Total PSA can be done for initial screening purposes. Most guidelines propose at the age of 50 years, although some recommend 45 years if there is a strong family history of cancer. If it is above 4 ug/L, then the test can be repeated to include the Free/Total PSA. However, if available, I prefer to do the PHI test (Prostate Health Index) which includes the Total PSA, Free PSA, and the PHI score. A score above 50 is highly suspect of cancer. The problem with PSA is that it can also be raised in those with large benign prostates (BPH) as well as prostatitis (inflammation).
Q: What’s BPH?
A: BPH refers to a benign enlarged prostate – the prostate gland is under the influence of testosterone and similar to the breast. Breast lumps are also caused by oestrogen and can be benign (majority) or cancerous.
Q: If prostate cancer is detected at an early stage, there are two main treatment methods – normal surgery and radiotherapy. Am I correct?
A: Early prostate cancer refers to cancer that is confined within the prostate. There are 3 options –
1) Active surveillance – this is applicable for low-risk, small cancers ( For example Gleason score of 6 detected in older men above 75 years
2) Radiotherapy – either external beam or proton beam or Brachytherapy (radiation seeds planted into the prostate.)
3) Surgery – either open, pure laparoscopic, or robotic.
Q: Could you elaborate on open surgery, laparoscopic surgery, and robotic surgery?
 A: Open surgery requires a long midline incision and the main difficulty is the bleeding while cutting out the prostate. Hence, the blood transfusion rate is as high as 70 percent.
A: Open surgery requires a long midline incision and the main difficulty is the bleeding while cutting out the prostate. Hence, the blood transfusion rate is as high as 70 percent.
Also, the reconstruction of the bladder to the urethra is difficult and not water-tight – resulting in a longer catheter time which can be as long as 2 weeks. If there is a leak, the catheter may have to be left in for even a month. Laparoscopy has the advantage of less bleeding, but is difficult to master and the suturing takes a longer time because of the limitation of the instruments. Robotic surgery overcomes this limitation because of the dexterity of the robotic instruments. The 3-dimensional, 10-times magnified camera also gives better vision and articulate dissection. Hence, blood loss is the least and the patient’s recovery is faster. It is the gold standard surgery for prostate cancer. The other advantage is to the surgeon – the surgeon is seated comfortably and able to focus on the surgery without physical strain or fatigue. The surgery can be done in as fast as 2 hours and he can even do 2 to even 3 cases a day with consistent outcome.
Q: Is chemotherapy only used for Stage 3 and 4 cancers?
A: Once the cancer goes out of the prostate, the cure is no longer possible. Hence, the alternative is radiation and this has to be combined with hormonal treatment which works by driving the testosterone level down, i.e. medical castration. The problem with medical castration is that after a few years, the cancer cells mutate and no longer respond to anti-testosterone treatment. Chemotherapy is then needed and the prognosis is limited.
Q: What are the latest treatment methods available at Mount Elizabeth Hospital to treat prostate cancer?
A: The hospital has the latest da Vinci Xi model which makes prostatectomy easier to do as well as the proton beam machine to deliver radiotherapy with less collateral damage to the rectum and bladder.
****
Key Points
* Prostate Cancer is the second most common cancer in men across the word
* Prostate cancer is quite rare before the age of 50 years.
* Prostate cancer is now detected at an early stage as a result of health screening.
* The diagnosis is suspected when the PSA is > 4 ug/L and confirmed from prostate biopsies.
* MRI can be done before biopsy to look for suspicious areas and facilitate fusion biopsy
* Treatment choices vary from active surveillance, surgery to radiotherapy.
* Surgery still gives the best cure rate ( > 90 percent cure ) and the robotic method is now the preferred choice because of faster recovery of continence, better preservation of potency, and lower chance of leaving cancer behind.
